Tissue hypoperfusion markers and their prognostic value in the mortality of critically ill patients in a multipurpose unit.
Article Sidebar
Main Article Content
Abstract
Introduction: Early detection of tissue hypoperfusion is crucial for the prognosis of critically ill patients. Traditional hemodynamic markers, such as lactate, the venoarterial carbon dioxide gradient (Delta PCO2), and central venous oxygen saturation (SvcO2), allow the assessment of different domains of cellular perfusion and cardiac output. The objective of this study was to correlate serum lactate, Delta PCO2, and SvO2 levels with mortality in critically ill patients treated in a polyvalent unit.
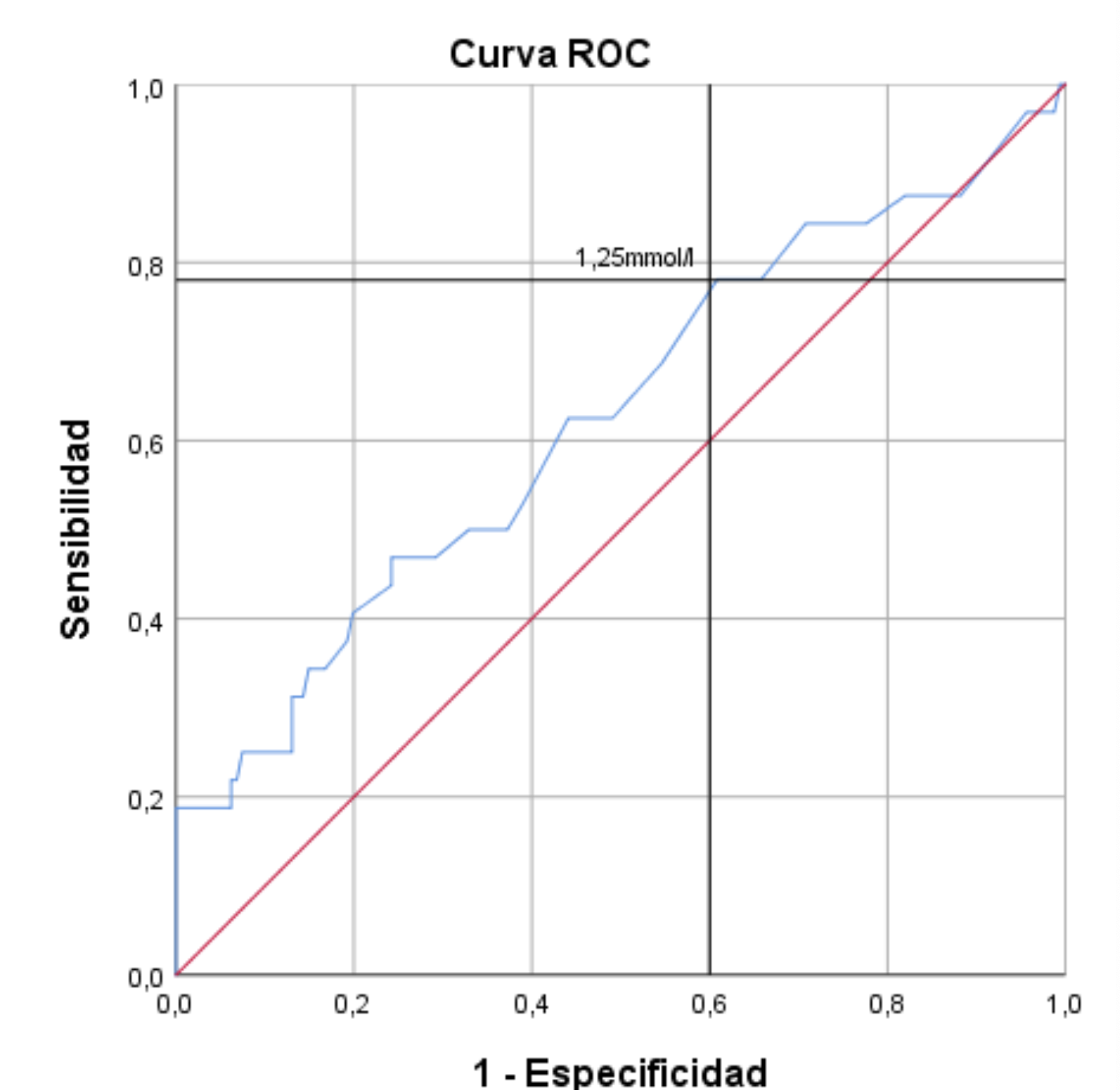
Methodology: An observational and analytical study was conducted at Alcívar Hospital in 2024, with a sample of 193 patients. Demographic, clinical (surgical vs. clinical pathology), and physiological variables (lactate, Delta PCO2, SvCO2, and APACHE II scale) were collected. The statistical analysis included measures of central tendency, Pearson correlation, bilateral significance, and diagnostic performance, as measured by the area under the ROC curve (AUC), to assess sensitivity and specificity with respect to mortality.
Results: The sample showed a predominance of males (67.4%) and surgical patients (81.4%), with an overall mortality of 16.5%. Delta PCO2 was the most frequently altered marker (>6 mmHg in 58.5% of cases) and was significantly associated with the APACHE II scale (rho = 0.039). However, lactate demonstrated the best diagnostic performance for mortality (AUC = 0.625), with an optimal cutoff of 1.25 mmol/l, yielding a sensitivity of 78% and a specificity of 61%. Mortality was significantly higher in medical patients (41.7%) than in surgical patients (10.8%; P < 0.0001), whereas SvcO2 did not show significant discriminative capacity in this sample.
Conclusions: Serum lactate is confirmed as the most sensitive predictor of mortality, even at borderline levels (1.25 mmol/l). Although Delta PCO2 is a frequent indicator of hemodynamic alteration in critically ill patients, its use should be complementary. Close multiparametric monitoring is recommended, especially in patients with a clinical profile, to guide timely resuscitation and reduce mortality rates in the intensive care unit.
Downloads
Article Details

This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License.